Can IVF Embryo Grading Improve Success Rates?
Quick Answer
Yes, IVF embryo grading helps embryologists identify embryos with the highest developmental potential and may improve embryo selection during IVF treatment. However, embryo grading alone cannot guarantee pregnancy. Factors such as embryo genetics, maternal age, uterine receptivity, sperm quality, and overall reproductive health significantly influence IVF success. Embryo grading should therefore be viewed as an important decision-making tool rather than a predictor of guaranteed outcomes.
Key Facts Table
| Factor | Details |
|---|---|
| Procedure | IVF Embryo Grading |
| Purpose | Evaluate embryo quality |
| Performed By | Embryologists |
| Assessment Days | Day 3 and Day 5/6 |
| Common System | Blastocyst Grading |
| Best Known Grades | AA, AB, BA |
| Predicts Pregnancy? | Partially |
| Predicts Genetics? | No |
| Used In | IVF, ICSI, IMSI |
| Helps Selection? | Yes |
Introduction
For most couples undergoing IVF, one of the most emotional moments occurs when they receive an update from the embryology laboratory. Questions such as “How many embryos formed?”, “Which embryo is best?” and “What are our chances?” are common.
To answer these questions, fertility specialists rely on embryo grading.
Embryo grading is a standardized laboratory assessment used to evaluate how embryos are developing after fertilization. The process helps embryologists determine which embryos appear healthiest and which may have the highest implantation potential.
Many patients incorrectly assume that an excellent embryo grade guarantees pregnancy or that a lower-grade embryo cannot produce a healthy baby. Neither assumption is true.
Understanding embryo grading can help patients make informed decisions and reduce unnecessary anxiety during IVF treatment.
What Is IVF Embryo Grading?
IVF embryo grading is a standardized laboratory assessment used to evaluate embryo development after fertilization. After eggs and sperm are combined through conventional IVF or ICSI treatment, embryologists monitor embryo growth and quality over several days.
After fertilization, embryos are carefully monitored in the IVF laboratory. Embryologists assess:
• Cell number
• Cell symmetry
• Fragmentation
• Growth rate
• Blastocyst formation
• Inner cell mass quality
• Trophectoderm quality
The objective is to identify embryos that have the greatest likelihood of resulting in implantation and pregnancy.
Embryo grading evaluates morphology (appearance) rather than chromosomal normality.
Who Needs Embryo Grading?
Embryo grading is routinely performed for patients undergoing:
• Conventional IVF Treatment
• ICSI Treatment
• IMSI Treatment
• Frozen Embryo Transfer
• Donor Egg IVF
• Blastocyst Transfer
• PGT-A Cycles
• Fertility Preservation Cycles
It becomes particularly important for women with reduced ovarian reserve, recurrent implantation failure, advanced maternal age, or couples pursuing fertility treatment at a specialized Ahmedabad fertility center
How Embryos Develop After Fertilization
Understanding embryo grading begins with understanding embryo development.
Day 1
Fertilization occurs.
Day 2
Embryo contains approximately 2–4 cells.
Day 3
Embryo typically reaches 6–8 cells.
Day 4
Compaction stage begins.
Day 5
Blastocyst stage develops.
Day 6
Further blastocyst expansion occurs.
Most modern IVF programs prefer evaluating embryos at the blastocyst stage because more developmental information becomes available.
Day-3 Embryo Grading
Day-3 embryos are evaluated according to:
Cell Number
Ideally 6–8 cells.
Symmetry
Cells should be relatively equal in size.
Fragmentation
Lower fragmentation is preferred.
Growth Pattern
Development should follow expected timelines.
Embryos demonstrating good growth and minimal fragmentation generally receive better grades.
Blastocyst Grading Explained
Blastocyst grading is currently one of the most widely used embryo assessment systems.
Today, many fertility specialists prefer blastocyst-stage assessment because it provides more information about embryo development.
If you are unfamiliar with blastocysts, read our detailed guide on Blastocyst Culture of Embryos, which explains why Day-5 embryo transfer has become increasingly common in modern IVF.
A blastocyst grade typically contains:
A number + two letters
Example:
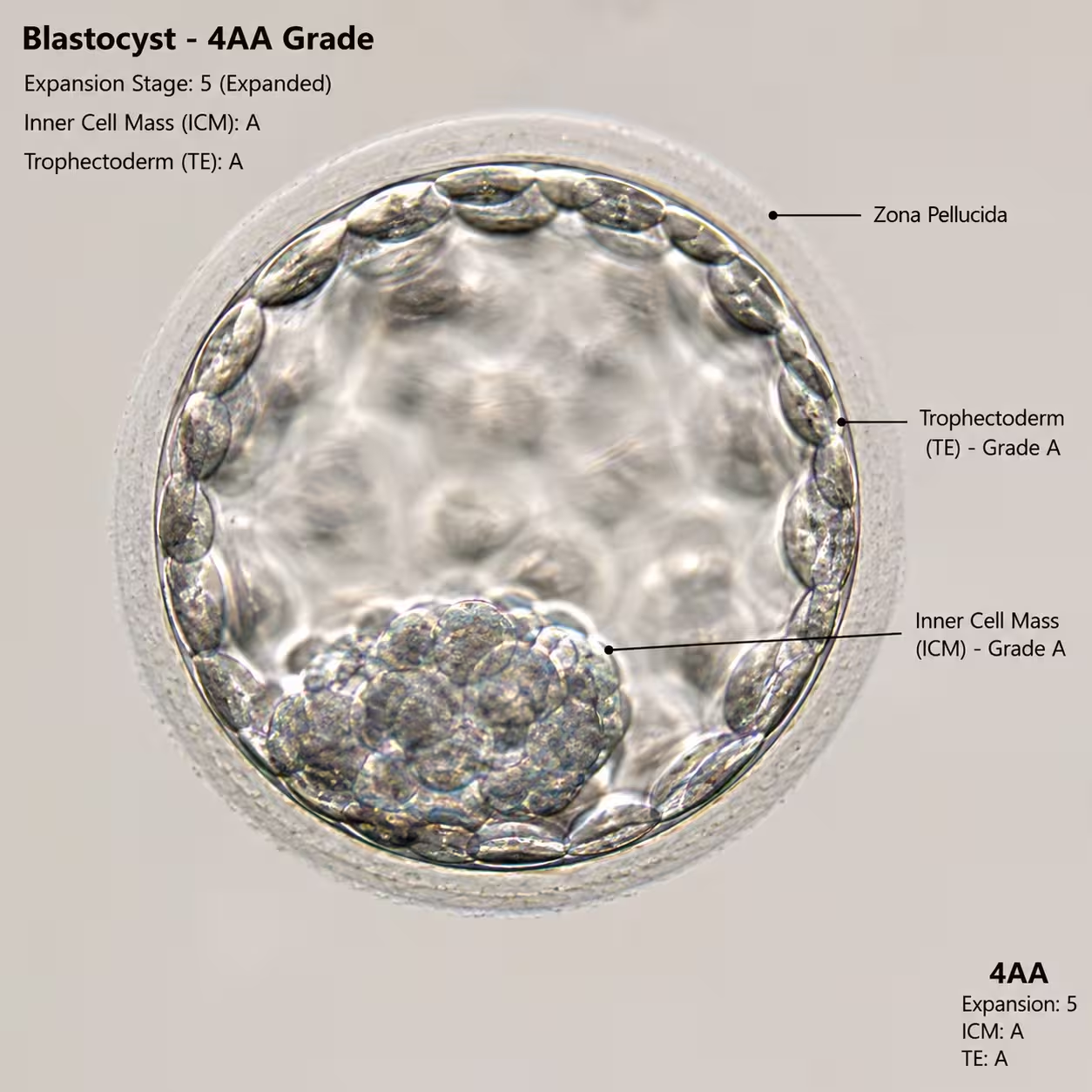
4AA
Expansion Score
The number represents blastocyst expansion.
1–6 grading scale is commonly used.
Inner Cell Mass (ICM)
First letter.
Represents cells that eventually form the fetus.
A = Excellent
B = Good
C = Lower quality
Trophectoderm (TE)
Second letter.
Represents cells that eventually form the placenta.
A = Excellent
B = Good
C = Lower quality
What Do Common Embryo Grades Mean?
| Grade | Interpretation |
| 5AA | Excellent |
| 4AA | Excellent |
| 4AB | Very Good |
| 4BA | Very Good |
| 4BB | Good |
| 3BB | Fair-Good |
| 3BC | Fair |
| CC | Lower Quality |
Although AA embryos are generally preferred, BB embryos frequently result in healthy pregnancies.
How Embryo Grading Influences Success Rates
Studies consistently show that higher-quality embryos tend to have:
• Better implantation rates
• Better clinical pregnancy rates
• Better live birth rates
However, embryo grading alone does not determine success.
Pregnancy depends on multiple biological factors.
Other Factors That Influence IVF Success
Female Age
Age remains one of the strongest predictors of IVF outcomes.
Embryo Genetics
A beautiful embryo may still contain chromosomal abnormalities.
Endometrial Receptivity
The uterus must be receptive at the time of transfer.
Sperm Quality
Poor sperm quality can affect embryo development.
Laboratory Quality
Advanced embryology laboratories generally produce better outcomes.
Medical Conditions
PCOS, endometriosis, adenomyosis, fibroids, thyroid disorders, and autoimmune conditions may influence implantation.
Advantages of Embryo Grading
Non-Invasive
No damage to the embryo.
Better Embryo Selection
Helps identify promising embryos.
Improved Transfer Strategy
Supports single embryo transfer.
Better Freezing Decisions
Helps determine which embryos should be cryopreserved.
Improved Counseling
Provides useful information for patient discussions.
Limitations of Embryo Grading
Does Not Assess Genetics
Embryo appearance is not equivalent to chromosomal normality.
Subjective Variation
Different embryologists may occasionally interpret findings differently.
Cannot Guarantee Pregnancy
Even perfect-looking embryos can fail.
Lower-Grade Embryos May Succeed
Embryo grading predicts probability, not certainty.
Embryo Grading vs PGT-A (Preimplantation Genetic Testing)
Many patients confuse embryo grading with genetic testing.
| Embryo Grading | PGT-A |
| Assesses appearance | Assesses chromosomes |
| Non-invasive | Requires biopsy |
| Evaluates morphology | Evaluates genetics |
| Lower cost | Additional cost |
| Useful for all cycles | Selected patients |
The two approaches often complement each other.
How Patients Can Improve Embryo Quality
While not every factor is controllable, several steps may improve reproductive health:
• Maintain healthy BMI
• Stop smoking
• Limit alcohol
• Optimize sleep
• Manage stress
• Treat hormonal disorders
• Address sperm DNA fragmentation
• Follow fertility specialist recommendations
• Use supplements only when medically advised
Clinical Insight From Dr. Pranay Shah
In my fertility practice at Wellspring IVF & Women’s Hospital, Ahmedabad, I frequently meet couples who become worried after hearing that their embryos are graded BB rather than AA.
One of the most important lessons I have learned over the years is that embryo grading is a useful guide but not a crystal ball. I have seen AA embryos fail to implant and BB embryos result in healthy babies. Successful IVF treatment depends on the interaction between embryo quality, genetics, uterine receptivity, laboratory excellence, and individualized treatment planning.
Patients should focus on the overall treatment strategy rather than a single embryo grade. Patients can better understand the complete treatment process by reading The Complete IVF Timeline: Day by Day
Common Myths About Embryo Grading
Myth 1:
AA embryos always become pregnancies.
Reality:
Even excellent embryos may fail to implant.
Myth 2:
BB embryos cannot produce healthy babies.
Reality:
Many successful pregnancies originate from BB embryos.
Myth 3:
Embryo grading evaluates chromosomes.
Reality:
It evaluates appearance, not genetics.
Myth 4:
Poor-grade embryos are always useless.
Reality:
Some lower-grade embryos still result in live births.
Myth 5:
Embryo grading guarantees IVF success.
Reality:
No grading system can guarantee pregnancy.
Recent Advances in Embryo Selection
Modern IVF laboratories now use:
• Time-lapse embryo monitoring
• AI-assisted embryo assessment
• Improved culture media
• Advanced incubator systems
• PGT-A integration
• Non-invasive embryo assessment research
These technologies continue to improve embryo selection and treatment outcomes.
Related Fertility Resources
You may also find these resources helpful:
• IVF Treatment [Internal Link: /treatments/ivf/]
• ICSI Treatment [Internal Link: /treatments/icsi-treatment/]
• IMSI Treatment [Internal Link: /treatments/imsi/]
• Blastocyst Culture of Embryos [Internal Link: /treatments/blastocyst-culture-of-embryo/]
• What Happens in the IVF Laboratory? [Internal Link: /blog/ivf-laboratory-embryology-explained/]
• The Complete IVF Timeline [Internal Link: /blog/ivf-timeline-day-by-day/]
• IUI vs IVF: When to Switch? [Internal Link: /blog/iui-vs-ivf-when-to-switch/]
• Blog Hub
Frequently Asked Questions
1. What is a good embryo grade in IVF?
Grades such as 5AA and 4AA are generally considered excellent quality blastocysts.
2. Can a BB embryo become a healthy baby?
Yes. Many successful pregnancies occur using BB-grade embryos.
3. Does embryo grading guarantee pregnancy?
No. It only estimates developmental potential.
4. What is blastocyst grading?
It is the evaluation of Day-5 or Day-6 embryos.
5. Can poor-quality embryos implant?
Yes, although implantation rates may be lower.
6. Which embryo grade is best?
AA grades are generally considered highest quality.
7. Does maternal age affect embryo quality?
Yes. Embryo quality and chromosomal normality typically decline with age.
8. Does sperm quality influence embryo grading?
Yes. Severe male-factor infertility may affect embryo development.
9. Is embryo grading subjective?
Some variability exists, although standardized systems reduce differences.
10. Can frozen embryos be graded?
Yes. Embryos are graded before freezing.
11. Should all patients undergo PGT-A?
No. The decision depends on age, history, and clinical circumstances.
12. What is the difference between AA and BB embryos?
AA embryos generally demonstrate superior morphology.
13. Can lifestyle affect embryo quality?
Healthy lifestyle choices may positively influence reproductive outcomes.
14. Is Day-5 transfer better than Day-3 transfer?
Many clinics prefer blastocyst transfer, although treatment is individualized.
15. What should I ask my fertility specialist about embryo grading?
Ask about embryo quality, transfer strategy, freezing plans, and whether additional testing may be beneficial.
Key Takeaways
• Embryo grading helps identify embryos with higher developmental potential.
• Blastocyst grading is the most commonly used assessment system.
• Embryo grading evaluates appearance, not genetics.
• AA embryos generally perform better statistically but do not guarantee pregnancy.
• Lower-grade embryos can still result in healthy babies.
• IVF success depends on multiple factors beyond embryo grade.
• Embryo grading should always be interpreted by an experienced fertility specialist.
Conclusion
Embryo grading is an important component of modern IVF treatment and helps embryologists select embryos with the greatest developmental potential. However, it represents only one part of the fertility journey. Genetics, maternal age, uterine health, sperm quality, and laboratory standards all contribute significantly to treatment outcomes.
Patients should view embryo grading as a valuable clinical tool rather than a guarantee of success or failure. A personalized treatment plan developed by an experienced fertility specialist remains the most effective approach to maximizing IVF outcomes.


{kind=link}