Poor Sperm Motility Treatment in Ahmedabad — Speed and Direction Matter
The Number on Your Report That Actually Matters
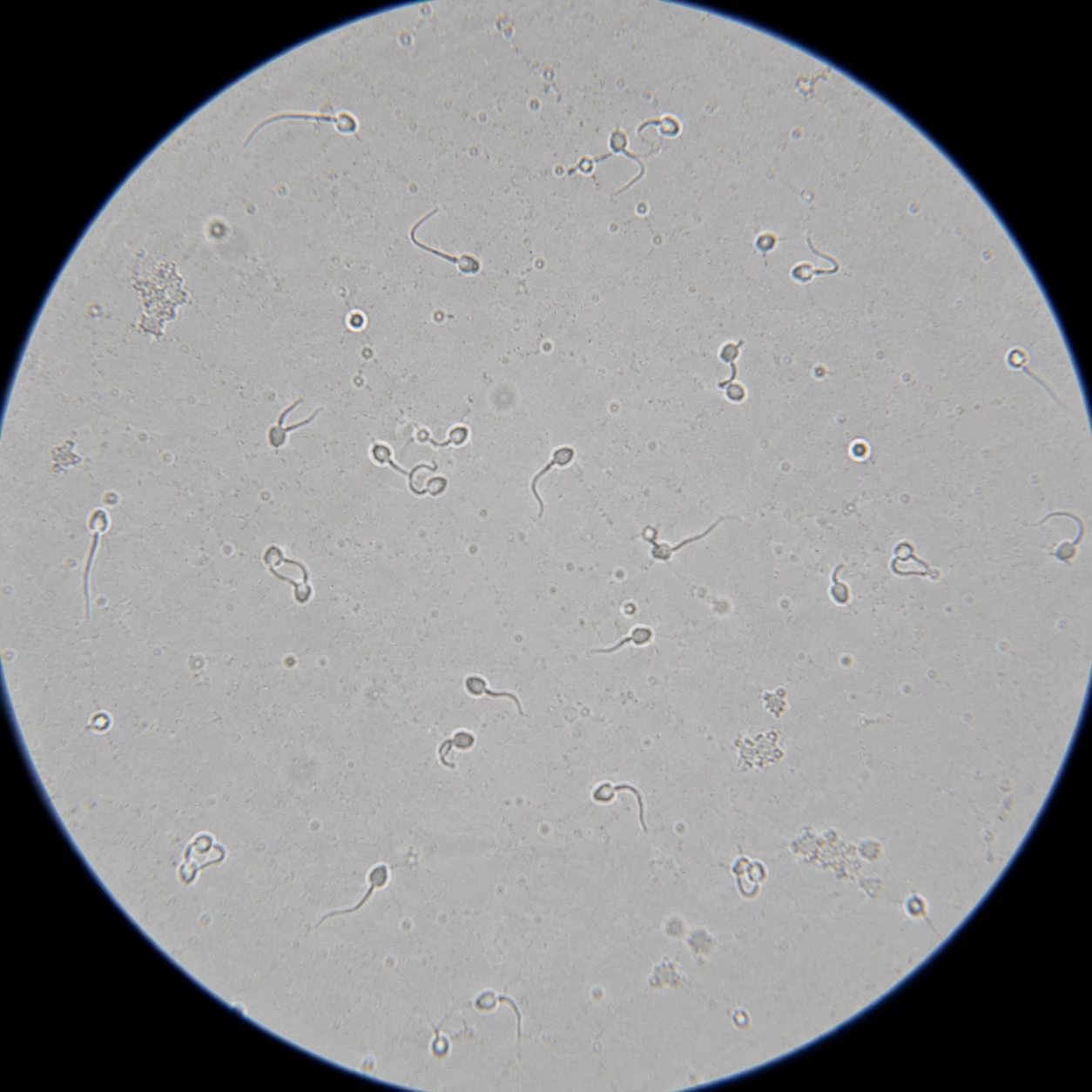
Your report says ‘Motility: 45%.’ That sounds fine.
But read further: ‘Progressive Motility: 18%.’
WHO normal for progressive motility is 32% or above. 18% means fewer than 1 in 5 sperm can actually swim toward the egg. The other 27% that are ‘motile’ are moving — but not forward. They cannot fertilise.
Poor Sperm Motility — At a Glance
| Poor Sperm Motility — At a Glance | |
|---|---|
| Medical Term | Asthenospermia (also Asthenozoospermia) — from Greek: asthenos (weak) + sperma (sperm) |
| WHO Normal Range | Progressive Motility (PR) ≥32% | Total Motility (PR + NP) ≥40% |
| What It Means | Sperm cannot swim strongly enough or in the right direction to reach and penetrate the egg naturally |
| Total vs Progressive | Total Motility = any movement (including twitching in place). Progressive Motility = forward-swimming in a straight or large curve — the only type that matters for fertilisation. |
| Severity — Mild | Progressive Motility 25–32% | Usually manageable with lifestyle + IUI |
| Severity — Moderate | Progressive Motility 10–25% | IUI with sperm preparation or early IVF |
| Severity — Severe | Progressive Motility <10% | ICSI strongly recommended — injects single sperm directly into egg |
| Asthenospermia Alone | Pure asthenospermia (normal count, low motility) is less common — most cases have combined parameters affected |
| Reversible Causes | Varicocele, oxidative stress, heat exposure, poor lifestyle — all improvable |
| Irreversible Causes | Kartagener syndrome (immotile cilia), severe sperm DNA damage — ICSI remains effective |
| Key Test | Semen Analysis (SA) — WHO 2021 criteria. Repeat after 72 hours abstinence, processed within 1 hour. Two tests 4–6 weeks apart |
| Consultation | 📞 9099946050 | Confidential, professional male fertility consultation |
Progressive vs Total Motility — The Distinction Your Report May Not Explain
This is the single most important concept for any man with a motility finding on his semen analysis. Understanding it correctly determines whether your treatment plan is appropriate — or whether it is addressing the wrong number.
| Movement Type | WHO Category | What It Looks Like | Fertility Significance |
|---|---|---|---|
| Rapid Progressive (a) | Category A [PR] | Sperm swimming rapidly forward in a straight line or large smooth curve. Speed ≥25 micrometres/sec. The ‘ideal’ swimmer. | Highest — can reach the egg and penetrate the zona pellucida |
| Slow Progressive (b) | Category B [PR] | Sperm moving forward but slowly or in a curved/erratic path. Speed <25 micrometres/sec. Still directional. | Good — contributes to fertilisation, less efficient than (a) |
| Non-Progressive (c) | Category C [NP] | Sperm moving but NOT going anywhere — vibrating, twitching, spinning in tight circles. No net forward movement. | Cannot fertilise — no forward progress toward the egg |
| Immotile (d) | Category D [IM] | Completely still. No movement at all. Note: immotile sperm may be alive (viable) or dead — HOS test distinguishes the two. | Cannot fertilise naturally — ICSI may use viable immotile sperm |
What Your Report Should Show — The Critical Numbers:
Total Motility = Category A + B + C (PR + NP). WHO normal: ≥40%
Progressive Motility = Category A + B (PR only). WHO normal: ≥32%
If your report shows only ‘Motility: X%’ without separating progressive from total — request a detailed WHO-graded semen analysis. The total number conceals the most important clinical information.
Reading Your Semen Analysis — Normal vs Mild vs Moderate vs Severe
| Parameter | WHO Normal | Mild | Moderate | Severe |
|---|---|---|---|---|
| Progressive Motility | ≥32% | 25–32% | 10–25% | <10% |
| Total Motility | ≥40% | 32–40% | 20–32% | <20% |
| Sperm Count | ≥16 million/mL | Usually normal | May be reduced | Often co-reduced |
| Morphology (normal forms) | ≥4% (Kruger strict) | Usually normal | May be reduced | Often <2% |
| Vitality (live sperm) | ≥54% | Usually normal | May be reduced | May be <40% |
| Clinical significance | Natural conception likely possible | IUI candidate | IUI/IVF borderline | ICSI strongly advised |
Causes of Poor Sperm Motility — What Is Affecting Your Sperm's Ability to Swim?
Causes of Asthenospermia — Reversible and Irreversible
Varicocele (most important reversible cause)
Dilated veins in the scrotum that raise testicular temperature and create venous reflux of toxic metabolites. The #1 surgically correctable cause of asthenospermia. Found in approximately 30–40% of infertile men with motility issues. Varicocele repair (varicocelectomy or percutaneous embolisation) improves progressive motility in the majority of cases within 3–6 months.
Oxidative Stress (OS) — The Most Common Biochemical Cause
Reactive oxygen species (ROS) — free radicals generated by immature sperm cells, white blood cells in semen (leukocytospermia), smoking, alcohol, environmental toxins, and obesity — directly damage the sperm flagellum’s axonemal structure and deplete mitochondrial ATP production. Oxidative stress is identifiable on a Reactive Oxygen Species test and is directly treatable with targeted antioxidants.
Heat Exposure
The testes require a temperature 2–3°C below core body temperature for optimal sperm production and motility. Prolonged laptop use on the lap, hot baths/saunas, sedentary desk jobs (prolonged sitting), tight underwear, and occupational heat exposure (bakers, welders, long-haul drivers) all increase scrotal temperature. The motility impact reverses within one full spermatogenesis cycle — approximately 74 days — after heat exposure is reduced.
Infection and Leukocytospermia
Genital tract infections (epididymitis, prostatitis, seminal vesiculitis) and subclinical infections increase white blood cell (WBC) concentration in semen > 1 million WBC/mL (leukocytospermia). WBCs generate massive oxidative stress directly within the seminal fluid, significantly reducing motility. Diagnosed on semen analysis + semen culture. Treated with targeted antibiotics.
Poor Lifestyle — Diet, Alcohol, Smoking
Smoking reduces progressive motility by 15–20% and increases sperm DNA fragmentation. Chronic alcohol use suppresses testosterone and impairs mitochondrial function. Micronutrient deficiencies — particularly zinc, selenium, coenzyme Q10, vitamin C, vitamin E, and L-carnitine — all directly impair flagellar energy production. These are modifiable. Three months of structured lifestyle change consistently improves progressive motility in mild-moderate cases.
Sperm DNA Fragmentation
High DNA Fragmentation Index (DFI >25%) is associated with poor motility because the same oxidative stress that damages DNA also damages the flagellar proteins responsible for movement. Importantly, sperm with high DNA damage may appear motile under standard microscopy — which is why DFI testing is a separate, important investigation in asthenospermia cases.
Kartagener Syndrome / Primary Ciliary Dyskinesia (PCD)
A rare genetic condition (1 in 20,000) in which the dynein arm proteins responsible for flagellar movement are structurally absent or defective. Results in complete sperm immotility (100% immotile sperm). These sperm are alive (viable on HOS test) but cannot move. Diagnosis: electron microscopy of sperm + genetic testing. Treatment: ICSI using viability-selected immotile sperm — successful pregnancies are well-documented with this approach.
Antisperm Antibodies (ASA)
IgG or IgA antibodies (produced after testicular trauma, vasectomy reversal, or infection) bind to the sperm head or tail and impair motility by agglutination and direct flagellar interference. Detected on MAR test or Immunobead test in semen analysis. High ASA levels (>50% binding): ICSI is the treatment of choice.
Ductal Obstruction Causing Stasis
Partial obstruction of the epididymis or ejaculatory ducts causes sperm stasis — prolonged transit time in an environment that depletes motility. Presents as asthenospermia with normal testicular function. Diagnosed on scrotal Doppler + semen analysis pattern. May be amenable to surgical correction.
What Our Patients Say


A special thank you to Dr. Pranay Shah for his confidence, guidance, and the way he explained everything so patiently. His positive approach gave me so much strength, and today I am blessed with my baby.
Thank you to each and every member of the hospital for taking such great care of me and supporting me throughout this journey. Forever grateful. 💕

He is, without a doubt, the most patient doctor I have ever met. Of course, treatment can be done by many. What truly sets him apart is his maturity, the way he pauses, explains, comforts, and most importantly, seeks your permission before moving forward. You never feel rushed. You never feel unheard. You feel respected.
And the staff deserves equal appreciation. They handle even the most anxious and impatient moments with such calm grace and dignity that you slowly find your own heartbeat settling down. It feels less like a clinic and more like a safe space.
I wholeheartedly recommend him to anyone who overthinks, seeks reassurance, or simply needs a doctor who believes comfort is the first step of healing. With him, care begins long before the treatment does.

Highly recommend for their expertise, kindness and dedication. "Turned out dream into reality"



Our gratitude also extends to everyone in your clinic who offered a smile, reassurance, technical support, or a listening ear along the way. We feel incredibly blessed to have chosen your practice for our journey, and we will always cherish the precious gift you helped us receive.
Thank you, from the bottom of our hearts, for making our dream a reality.
Join 750+ Satisfied Families
Diagnosis — Dr. Shah's Asthenospermia Workup
| Investigation | Purpose & What It Identifies |
|---|---|
| Detailed Semen Analysis (×2) | WHO 2021 graded parameters: volume, pH, count, progressive motility, total motility, morphology (Kruger strict), vitality, WBC count. Two samples 4–6 weeks apart for reliable baseline. |
| Sperm DNA Fragmentation Index (DFI) | SCSA (Sperm Chromatin Structure Assay) or SCD test. DFI <15% normal; 15–25% borderline; >25% associated with RPL and IVF failure. Essential in asthenospermia because OS affects both simultaneously. |
| Scrotal Doppler Ultrasound | Identifies varicocele (grade I–III), epididymal obstruction, testicular volume (proxy for reserve), and structural abnormalities. |
| Semen Culture + Leukocyte Count | Identifies bacterial infection and leukocytospermia (>1M WBC/mL). Critical if WBC are elevated on routine SA — guides antibiotic choice. |
| Hormone Panel (FSH, LH, Testosterone, Prolactin) | Distinguishes primary testicular failure from secondary (pituitary/hormonal). Low testosterone with low LH/FSH: hypogonadotropic hypogonadism — treatable with gonadotropin therapy. |
| HOS Test (Hypoosmotic Swelling Test) | Distinguishes viable (membrane-intact) immotile sperm from dead sperm. Critical for planning ICSI in complete asthenospermia — viable immotile sperm can be used for ICSI with good outcomes. |
| Reactive Oxygen Species (ROS) Assay | Directly quantifies free radical levels in semen. Confirms oxidative stress as the primary mechanism — guides antioxidant therapy selection. |
| MAR Test / Immunobead Test | Detects antisperm antibodies (ASA). If >50% of motile sperm carry antibodies: ICSI is the treatment of choice. |
| Genetic Testing (if indicated) | Karyotype, Y-chromosome microdeletion, CFTR mutation. In complete asthenospermia with suspected PCD: TEM electron microscopy. |
The Treatment Ladder — Dr. Shah's Graduated Approach to Asthenospermia
Not every case of poor sperm motility requires IVF. Dr. Shah’s principle: start with the least invasive effective intervention and escalate only when the clinical picture requires it. The severity of asthenospermia, the partner’s fertility status, couple’s age, and time-to-pregnancy goals all determine which step to start from:
Lifestyle Optimisation & Targeted Antioxidant Therapy
The 74-day principle: Spermatogenesis — the complete process of sperm production from stem cell to ejaculated sperm — takes 74 days. This means any intervention (antioxidants, lifestyle, varicocele repair) must be maintained for a minimum of 74–90 days before a repeat semen analysis is meaningful. Men who retest at 4 weeks are measuring the old cohort of sperm. Patience is not optional — it is biological
Antioxidant protocol — evidence-based combination: Coenzyme Q10 (200–300mg/day) — mitochondrial energy production in flagellum. Vitamin C (1000mg/day) + Vitamin E (400IU/day) — neutralise ROS directly. L-Carnitine / Acetyl-L-Carnitine (2–3g/day) — principal energy substrate for sperm motility. Zinc (25–50mg/day) + Selenium (100–200mcg/day) — structural integrity of flagellar proteins. Lycopene (4–8mg/day) — antioxidant with specific benefit in male infertility. Omega-3 fatty acids — membrane fluidity of sperm tail.
Lifestyle changes with direct motility evidence: Stop smoking: progressive motility improves 15–20% within 3 months. Reduce/eliminate alcohol: testosterone normalises within 4–8 weeks. Scrotal cooling: switch to loose-fitting cotton underwear, avoid prolonged sitting without breaks, no laptop on lap. BMI optimisation: obesity-related hypoestrogenism suppresses testosterone and directly reduces motility. Sleep: chronic sleep deprivation reduces testosterone by 10–15%.
Infection treatment (if leukocytospermia found): Targeted antibiotic course (doxycycline or fluoroquinolone based on culture) combined with antioxidant therapy. Repeat SA + culture 6 weeks post-treatment.
Varicocele Repair
Who benefits: Men with: clinical varicocele confirmed on Doppler, progressive motility <32%, no other azoospermia (absent sperm) diagnosis, and female partner with no significant fertility issues. Varicocele repair is not recommended when the female partner has severe tubal disease or advanced age — the 6–9 month wait for sperm improvement may not be in the couple’s best interest.
The procedure — microsurgical varicocelectomy: Subinguinal microsurgical varicocelectomy is the gold-standard technique. Performed under magnification, the dilated testicular veins are ligated while preserving the testicular artery and lymphatics. Day procedure. Recovery 1–2 weeks. Complication rate <5% in experienced hands.
Expected outcomes: Improvement in progressive motility: 60–70% of men show significant improvement within 3–6 months. Natural conception rate post-varicocelectomy in couples with no other fertility factors: approximately 30–40% within 12 months. Sperm DNA fragmentation also typically improves significantly after repair — as the source of oxidative stress (venous reflux) is eliminated.
IUI — Intrauterine Insemination
How IUI bypasses poor motility: In natural intercourse, sperm must travel from the vagina through cervical mucus, across the cervical canal, through the uterus, and up to the fallopian tube — a journey of 15–20 cm. Poor progressive motility often fails at the cervical mucus barrier. IUI deposits washed, concentrated, motility-selected sperm directly into the uterine cavity — eliminating the cervical barrier and reducing the swimming distance to <5cm.
Sperm preparation for IUI: Swim-up technique: only progressively motile sperm are selected. Density gradient centrifugation: separates motile sperm from non-motile, debris, and seminal fluid. After preparation: a small volume of highly concentrated, washed, progressively motile sperm is deposited via soft catheter into the uterine cavity.
IUI success rates in asthenospermia: Per cycle success rate: 10–15% (natural cycle) to 15–20% (with ovarian stimulation). Most benefit seen with: progressive motility ≥10% pre-wash, total motile count post-wash ≥5–10 million, female partner <35 with no significant issues. If 3 IUI cycles fail with no other cause: escalate to IVF/ICSI evaluation.
ICSI — The Ultimate Bypass for Severe Asthenospermia
Why ICSI is the game changer for motility problems: ICSI completely eliminates the sperm motility requirement. Instead of requiring sperm to swim to and penetrate the egg, Dr. Shah’s embryologist selects a single sperm under 200–400× magnification and injects it directly into the egg cytoplasm with a fine glass needle. The sperm never has to swim. Even a sperm with barely perceptible movement — or a viable but immotile sperm selected by HOS test — can successfully fertilise an egg via ICSI.
IMSI — for the most complex cases: IMSI (Intracytoplasmic Morphologically-Selected Sperm Injection)uses 6,000× magnification — approximately 20× higher than standard ICSI — to identify morphological defects in the sperm head and nucleus that are invisible under standard ICSI magnification. For men with severe asthenospermia combined with high DNA fragmentation or poor morphology, IMSI offers an additional layer of selection precision beyond standard ICSI.
ICSI success rates in asthenospermia: Fertilisation rate: 65–75% of mature eggs fertilised with ICSI — comparable to natural fertilisation rates in couples without male factor. Clinical pregnancy rate per transfer: 40–50% for good-quality blastocysts. The motility deficit is effectively neutralised — the embryo quality and uterine environment then become the determining factors.
When to go directly to ICSI without trying lower steps: Progressive motility <5%, total motility <15%. Complete asthenospermia (0% motility) with viable sperm on HOS. Kartagener syndrome / PCD. Antisperm antibodies >50% binding. Failed IUI after 3 cycles. Female partner age ≥37 — time does not permit waiting for lifestyle response. Combined male factor (asthenospermia + oligospermia + teratospermia).
Got Your Semen Analysis Report? Let Us Read It With You.
Your Fertility Consultant
Our fertility specialists are committed to providing personalized, compassionate care with
the latest reproductive medicine techniques.

Dr. Pranay Shah

Divyesh Bhalodia

Urmi Chauhan
Complete Asthenospermia — Zero Motility: Is There Still Hope?
The HOS Test — The Most Important Test You Have Never Heard Of
The Hypoosmotic Swelling (HOS) Test distinguishes between two very different situations:
Situation A — Sperm are alive but immotile. The sperm membrane is intact (viable), but the flagellar motor apparatus is not functioning — due to a structural defect (PCD/Kartagener), extreme oxidative damage, or severe antisperm antibody binding. HOS test result: positive (sperm tail curls in hypoosmotic solution). These sperm can be used for ICSI. The sperm does not need to move — it only needs to be alive and carry intact genetic material.
Situation B — Sperm are dead (necrospermia). The sperm membrane has ruptured — the cell is no longer viable. HOS test result: negative (tail does not curl). Dead sperm cannot be used for ICSI. In confirmed necrospermia: causes include severe epididymal dysfunction, systemic illness, or extreme oxidative stress. Investigation and treatment of the underlying cause — and, if necessary, testicular sperm extraction — are the next steps.
Key message: Complete asthenospermia with a positive HOS test is treatable with ICSI. Dr. Shah has achieved successful pregnancies in couples where the initial report showed 0% motility — using viability-selected immotile sperm.
“The most common mistake I see is a man who has been told ‘your motility is 42%, that’s fine’ — and nobody noticed the progressive motility was 14%. The total number looked acceptable. But only 14% of his sperm could actually swim forward. That’s the number that explains why they weren’t conceiving. Once we properly assessed the cause — varicocele in his case — and treated it with repair plus targeted antioxidants, progressive motility improved to 31% within 5 months. They conceived naturally.”
— Dr. Pranay Shah, MS (ObGy), Director & Chief Fertility Consultant, Wellspring IVF & Women’s Hospital, Ahmedabad
Frequently Asked Questions
My count is normal but motility is low — can I still conceive naturally?
Yes — depending on how low the progressive motility is and the female partner’s fertility status. Mild asthenospermia (PR 25–32%) with a young partner who has no female factor issues: natural conception is possible, though may take longer than average. Moderate asthenospermia (PR 10–25%): natural conception is unlikely without assistance — IUI or IVF/ICSI is recommended. Severe asthenospermia (PR <10%): ICSI is the recommended treatment for efficient, predictable results.
How long do antioxidants take to improve sperm motility?
A minimum of 74–90 days — one complete spermatogenesis cycle. Any semen analysis performed before this point measures sperm that were already in production before the supplements began. Dr. Shah requests a repeat SA at 3 months, then again at 6 months if improvement is partial. Men who stop supplements after 6 weeks because ‘it isn’t working’ are abandoning the treatment before the new cohort of improved sperm has been produced.
Does asthenospermia affect the health of the baby?
No. Poor motility is a transport problem — it affects the sperm’s ability to reach the egg, not the genetic quality of the sperm once it does. A baby conceived via ICSI using sperm with poor motility is no more at risk of genetic abnormalities than a baby conceived naturally. The exception: if the underlying cause of poor motility is high sperm DNA fragmentation — which is associated with miscarriage risk and should be separately assessed and treated.
What is the difference between asthenospermia and azoospermia?
These are completely different conditions. Asthenospermia = sperm are present but cannot swim well. Azoospermia = no sperm in the ejaculate at all. Azoospermia requires surgical sperm retrieval (TESE/PESA) for IVF/ICSI, whereas asthenospermia uses ejaculated sperm — just processed and selected differently based on severity.
Can varicocele repair completely cure asthenospermia?
In many cases, yes — particularly when varicocele is the primary cause. Studies show that microsurgical varicocelectomy improves progressive motility in 60–70% of men with clinical varicocele. Some men with moderate asthenospermia due to varicocele achieve complete normalisation of motility within 6 months and conceive naturally. Others show meaningful improvement that makes IUI effective where it previously was not. Dr. Shah advises varicocele repair as a genuine treatment — not just an investigative step — when the diagnosis is confirmed.
I have 0% motility on my report. Is there any hope?
Yes — and the answer depends on whether the sperm are alive but not moving, or dead. The HOS test makes this critical distinction. If your sperm are viable (positive HOS), Dr. Shah can use ICSI with viability-selected immotile sperm — and successful pregnancies are well-documented with this technique. If you have been told you have 0% motility, do not assume the outcome before the HOS test has been performed.
My wife's tests are all normal. Is poor motility the only reason we can't conceive?
It is the primary identified reason — but a full assessment of both partners simultaneously is always important. In approximately 20–25% of couples, both partners have a contributing factor. Dr. Shah assesses both partners at the first consultation — female evaluation (ovarian reserve, uterine cavity, tubes) is conducted in parallel with the male workup so that the complete picture is available before deciding on treatment.
Is ICSI safe? Will it affect fertilisation rates?
ICSI is the world’s most performed male infertility treatment — used in the majority of IVF cycles globally. Fertilisation rates with ICSI: 65–75% of mature eggs fertilised per cycle — comparable to or exceeding natural fertilisation rates. The procedure itself does not increase congenital abnormality risk above the background population rate. The data on ICSI outcomes are extensive — millions of healthy babies have been born globally via this technique since 1992.
Related Insights & Articles
 Can You Increase AMH Levels Naturally? What Science Says About Low AMH and Fertility Quick Answer In most cases, AMH…June 11, 2026
Can You Increase AMH Levels Naturally? What Science Says About Low AMH and Fertility Quick Answer In most cases, AMH…June 11, 2026- Things to Avoid After IUI: Complete Post-IUI Care Guide Direct Answer After IUI treatment, patients should avoid smoking, excessive alcohol…June 11, 2026
- Endometrial Scratching in IVF: Benefits, Procedure, Success Rates and Who May Need It Direct Answer Endometrial scratching, also known as…June 11, 2026